Epilepsy
Objective
At the end of PDF Notes, student will be able to
• Define epilepsy
• Define status epilepticus
• Classify epilepsy
• Describe the pathogenesis of epilepsy
Epilepsy
• Chronic brain disease of diverse etiology
• Characterized by recurrent paroxysmal episodes of uncontrolled excitation of brain neurons
• Manifesting as brief episodes (seizures) of loss of consciousness, with or without characteristic body movements (convulsions)
Status epilepticus (SE)
Continuous convulsion lasting longer than 30 minutes OR Occurrence of serial convulsions between which there is no return of consciousness
Pathophysiology of Epilepsy
• Normally, a balance between excitatory and inhibitory factors – proper functioning of a healthy human brain
• Reduction of inhibitory synaptic activity or enhancement of excitatory synaptic activity -trigger a seizure
• NTs mediating the bulk of synaptic transmission in the mammalian brain are amino acids
• GABA – principal inhibitory
• Glutamate – excitatory neurotransmitters
• Repeated epileptic discharge can cause neuronal death (excitotoxicity).
• A relative deficiency of inhibitory neurotransmitters such as GABA
• An increase in excitatory neurotransmitters such as glutamate would promote abnormal neuronal activity
Clinical manifestations of Epilepsy
• Depend on the location of the focus and the pathways involved in its spread
• ‘Generalised’ – initial activation of both hemispheres of the brain
• ‘Partial’ or ‘Focal’ – discharge starts in a localised area of the brain
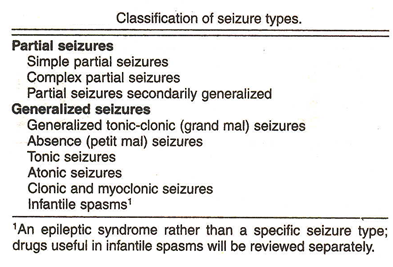
Grandmal seizure
• Generalized convulsion, also called the grand-mal seizure.
• Patient loses consciousness and usually collapses.
• Followed by generalized body stiffening (called the “tonic” phase of the seizure) for 30 to 60 seconds,
• violent jerking (the “clonic” phase) for 30 to 60 seconds,
• patient goes into a deep sleep.
• During grand-mal seizures, injuries and accidents may occur,
• Tongue biting and urinary incontinence
Absence seizures
• Short loss of consciousness (just a few seconds) with few or no symptoms
• Patient, most often a child
• Seizures begin and end abruptly
• Patients are usually not aware that they are having a seizure, except that they may be aware of “losing time.”
Myoclonic seizures
• Consist of sporadic jerks
• Usually on both sides of the body
• Patients sometimes describe the jerks as brief electrical shocks
• When violent, these seizures may result in dropping or involuntarily throwing objects
Clonic seizures
Repetitive
Rhythmic jerks
Involve both sides of the body at the same time
Tonic seizures
Tonic seizures are characterized by stiffening of the muscles.
Atonic seizures
• Sudden and general loss of muscle tone
• Particularly in the arms and legs
• Often results in a fall
Simple partial seizures
• Key feature is preservation of consciousness
• A sudden depolarization within a group of neurons called Paroxysmal depolarizing shift (pds)
• Lasts for 200 ms occurs in case of patients with partial seizures.
• This results in generation of an abnormally rapid train of action potentials
Complex partial seizure
• Impaired consciousness lasting 30 seconds to 2 minutes
• Often associated with purposeless movements such as lip smacking or hand wringing
• Associated with amnesia
Secondarily generalized seizure
Ø Partial seizures may get generalized
Ø spreading along diffuse connections to involve both cerebral hemispheres
Ø This seizure spread occurs through several pathways
ü U FIBRES connect various regions of the cortex.
ü CORPUS CALLOSUM allows for spread between hemispheres.
ü THALAMOCORTICAL PROJECTIONS provide a pathway for diffused synchronized spread throughout the brain
Summary
• Epilepsy is characterized by recurrent paroxysmal episodes of uncontrolled excitation of brain neurons
• Manifesting as brief episodes (seizures) of loss of consciousness, with or without characteristic body movements (convulsions)
• Continuous convulsion lasting longer than 30 minutes is status epilepticus
FAQ:
Q1: What is epilepsy? Epilepsy is a neurological disorder characterized by recurrent, unprovoked seizures. Seizures result from abnormal electrical activity in the brain, leading to various symptoms and altered consciousness.
Q2: Can you define status epilepticus? Status epilepticus is a medical emergency characterized by a prolonged and continuous seizure or a series of seizures without a full return to consciousness in between. It is a life-threatening condition that requires immediate medical attention.
Q3: How is epilepsy classified? Epilepsy is classified into different types based on various factors, including seizure characteristics, cause, and brain regions affected. Common classifications include focal (partial) epilepsy, generalized epilepsy, and epilepsy syndromes with specific features.
Q4: What is the pathogenesis of epilepsy? The pathogenesis of epilepsy involves abnormal electrical activity in the brain, which can result from various factors. These factors may include genetic predisposition, brain injuries, structural abnormalities, infections, or metabolic imbalances. Imbalances in neurotransmitters and ion channels can also contribute to the development of seizures.
Q5: What are the common triggers or causes of epilepsy? Epilepsy can be caused by a range of factors, including brain injuries (such as head trauma), brain tumors, genetic factors, infections like encephalitis, metabolic disorders, developmental issues, and in some cases, the cause may remain unknown (idiopathic).
Q6: What are the main types of seizures associated with epilepsy? Seizures in epilepsy can be classified into two main types: focal seizures, which start in one area of the brain, and generalized seizures, which involve the entire brain. Within these categories, there are various subtypes of seizures, each with distinct characteristics.
Q7: How is epilepsy diagnosed, and what are the key diagnostic tests? Diagnosis typically involves a detailed medical history, neurological examination, and various tests, such as electroencephalogram (EEG), magnetic resonance imaging (MRI), and blood tests. These tests help in confirming the diagnosis and identifying the specific type of epilepsy.
Q8: What is the role of medication in managing epilepsy, and are there other treatment options available? Medications, called antiepileptic drugs (AEDs), are often the first line of treatment for epilepsy. They help control seizures in many patients. In cases where medications are ineffective, other treatment options may include surgery, dietary therapies, and neurostimulation devices.
Q9: Can epilepsy be prevented or its impact minimized? While epilepsy itself is not always preventable, individuals can take measures to reduce the risk of head injuries, which can be a cause of epilepsy. Proper management and adherence to treatment plans can help minimize the impact of epilepsy on a person’s life.
Q10: What are the potential complications and challenges associated with epilepsy? Epilepsy can have various complications, including injuries during seizures, cognitive and psychological difficulties, and limitations on daily activities. Additionally, the stigma associated with epilepsy can pose social and emotional challenges for individuals with the condition.
