Parkinsons disease
Objectives
By the end of this PDF Notes, students will be able to:
a) Explain the pathophysiology of Parkinson’s disease
b) Describe the complications and symptoms of Parkinson’s disease
c) Explain the role of nigrostriatal pathway in the development of Parkinson’s Disease
Parkinson’s disease
Definition:
A neurological syndrome characterized by tremor, rigidity, hypokinesia and postural instability. As the symptoms progress patient may have difficulty in walking, talking or completing other simple tasks.
Disease is named after the English doctor James Parkinson, who published the first detailed description in “An Essay on the Shaking Palsy” in 1817
“Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported; with propensity to bend the trunk forward and to pass from walking to a running pace; the senses and the intellects being uninjured.”
Parkinsonism
Epidemiology:
- Approximately 15 per 100000 to 90 per 100000 are estimated to suffer from parkinsonism
- Less common in Asian countries
- Risk of developing during one’s lifetime 2-3 %
- The 2nd most common neurodegenerative disorder
Etiology & Pathogenesis of Parkinsons disease
Parkinsonism is either idiopathic or secondary
Idiopathic: Denotes a disease of unknown cause
Secondary: Only small amount of cases:
- Trauma induced
- Chemical induced- heavy metals, carbon monoxide, cyanide, pesticides, dyes, methyl chloride
- Drug induced- phenothiazines, reserpine, butyrophenol, large doses of carbamazepine
- Infection induced- syphilis, typhoid, herpes, encephalitis may mimic parkinsonism
- Tumour induced- Intracranial tumour
- Post cephalic- A sequel of the viral infection Encephalitis lethargica
Physiology of nigrostriatal pathways
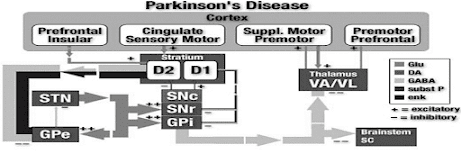
Anatomically, the basal ganglia form a re-entrant loop by
• Receiving the input from the cerebral cortex.
• Processing this information in the context of dopaminergic input from substantia nigra &
• Sending information back to the cortex by way of the thalamus.

The outflow of striatum proceeds along two distinct routes, identified as direct and indirect pathways, the balance of which regulates the movement.
DIRECT PATHWAY:
• It is also known as pyrimidal pathway.
• Formed by striatal neurons expressing primarily dopamine D1 receptors.
• These neurons projects directly to the output of the basal ganglia, the internal segment of the globus pallidus.
• These neurons tonically inhibit the thalamus, which in turn, sends excitatory projections to the cortex that initiate movement.

INDIRECT PATHWAY :
• It is also known as extrapyrimidal pathway.
• Formed by the striatal neurons expressing predominantly dopamine D2 receptors.
• These neurons projects to the external segment of the globus pallidus, which in turn inhibits the neurons in the subthalamic nuclei.
• The neurons in the subthalamic nucleus are excitatory glutaminergic neurons that project to the internal segment of the globus pallidus
• The indirect pathway inhibits movement.
• The differential expression of D1 & D2 receptors within the two pathways leads to differing effects of dopaminergic stimulation.
• Increased levels of dopamine in the striatum tend to activate the D1 expressing neurons of the direct pathway while
inhibiting the D2 expressing neurons of the indirect pathway. Both of these effects promote movement.
• The opposite effect is seen in PD, a state of dopamine deficiency: the direct pathway shows reduced activity while indirect
pathway is overactive, leading to reduced movement.
• In PD, neurons that extend from the substantia nigra to the putamen and caudate nucleus degenerate, causing the disruptions.
Ø Thus loss of nigrostriatal dopamine neurons in IPD results in reduction of cortical activation.
Ø Virtually all the motor deficits of IPD are attributable to the marked loss in dopaminergic neurons projecting to the
putamen.

• DA has a balance with the excitatory neurotransmitter Ach to initiate motor activities.
• Ach is secreted by cholinergic neurons present in synapses.
• When there is a loss of DA in Parkinsonism, balance is shifted to Ach. Over activity of Ach is responsible for the symptoms
of Parkinsonism.
Etiology & Pathogenesis of Parkinson’s disease
• Parkinsonism is either idiopathic (primary) or secondary parkinsonism.
• Unlike the idiopathic parkinsonism, many of the secondary forms of parkinsonism can be cured.
Idiopathic Parkinsonism
• The term “idiopathic “denotes a disease of unknown cause.
• Many theories have been proposed & each in succession has been abandoned because of lack of supporting evidence.
Ø Neurotoxins highly selective for substantia nigra pars compacta (SNc) dopaminergic neurons –
Ø 6-hydroxy dopamine
Ø MPTP(N-methyl 4-phenyl tetrahydropyridine)
Ø Cellular damage from oxyradicals.
Ø Dopamine – free radicals from autooxidation and from MAO metabolism
Secondary Parkinsonism
• It is either:
• Trauma induced- severe head injuries. They rarely produce Parkinson’s symptoms. usually occurs soon after injury & recovery is the general rule
• Chemical induced- acute ingestion of large amount of chemicals’ such as heavy metals, carbon monoxide, cyanide, pesticides, some photogenic dyes, methyl chloride can produce symptoms of Parkinsonism. But recovery is possible in most cases.
• Drug induced- phenothiazines commonly produce extra pyramidal effects that ultimately may manifest as Parkinsonism like syndrome. The true Parkinsonism like syndrome usually appears 2-3 months after initiation of drug therapy. Other drugs besides phenothiazines are haloperidol, butyrophenones, reserpine, large doses of methyl dopa, metochlopramide,carbamazipines.
• Infection induced- infection condition like syphilis, typhoid, herpes, coxsakie virus, Japanese encephalitis. Etc may mimic Parkinsonism complication.
Pathogenesis Parkinson’s disease
• A progressive neurodegenerative disorder
• The pathological hallmark of PD is a loss of the pigmented, dopaminergic neurons of the substantia nigra, with the appearance of intracellular inclusions known as Lewy bodies.
• Caused by degeneration of substantia nigra in the midbrain, and consequent loss of DA-containing neurons in the nigrostrial pathway
• Two balanced systems are important in the extrapyramidal control of motor activity at the level of the corpus striatum
and substantia nigra- first neurotransmitter – Ach & the second – D

- Neurons which produce the neurotransmitter dopamine in the area of brain substantia nigra die or become impaired
resulting in result in loss of DA - Lewy bodies are the pathological hallmark of the idiopathic disorder
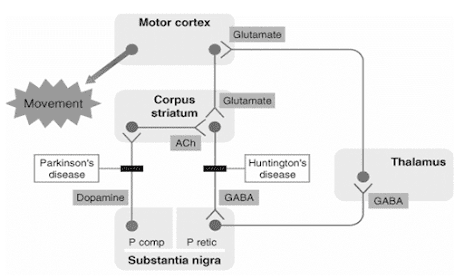
- Dopamine is responsible for transmitting signals b/w substantia nigra to next relay station of brain, the corpus striatum to produce smooth and co-ordinated muscle activity
- The symptoms of PD are connected with loss of nigrostrial neurons and DA depletion
- The cause of selective degeneration of nigrostrial neurones in PD
- is not precisely known, appears to be multifactorial
- Oxidation of DA by MAO-B and aldehyde dehydrogenase generate hydroxyl free radicals (˙OH) in the presence of
ferrous iron (basal ganglia are rich in iron) - Normally these radicals are quenched by glutathione and other endogenous antioxidants
- Age-related (e.g. in atherosclerosis) and/or otherwise acquired defect in protective antioxidant mechanisms
allows the free radicals to damage lipid membranes and DNA resulting in neuronal degenerations - Genetic predisposition may contribute to high vulnerability of substantia nigra neurons
- Environmental toxins or some infections may accentuate these defects
- A synthetic toxin N-methyl-4-phenyl tetrahydropyridine (MPTP), which occurs as a contaminant of some illicit
drugs, produces nigrostrial degenerations similar to PD - Neuroleptics and other DA blockers may cause temporary PD

Production of free radical by the metabolism of dopamine (DA)
DA is converted by MAO and aldehyde dehydrogenase (AD) in 3,4-dihydroxyphenylacetic acid (DOPAC), producing hydrogen peroxide (H2O2). In the presence of ferrous ion hydrogen per-oxide undergoes spontaneous conversion, forming a hydroxyl free
radical (The Fenton reaction).
Factors contributing to degeneration of nigrostrial DA-ergic neurones causing PD


The key steps in the synthesis and degradation of dopamine and the sites of action of various psychoactive substances at the dopaminergic synapse
Pathogenesis
- Nerve cells of striatum loose control in co-ordinate muscle activity
- DA has a balance with the excitatory neurotransmitter Ach in the corpus striatum , to initiate motor activities
- When there is a loss of DA in Parkinsonism , balance is shifted to Ach , therefore over activity of Ach is responsible for the symptoms of Parkinsonism.

Distribution and characteristics of DA receptors in the central nervous system

Complications
The disease is often accompanied by these additional problems, which are variably treatable
- Thinking difficulties
- Depression and Emotional changes
- Sleep problems and sleep disorder
- Bladder problems
- Constipation
- Sexual dysfunction
Symptoms of Parkinsonism
The signs of advanced Parkinsonism are so striking and unique that it hardly ever possses a diagnostic challenge.
The symptoms are connected with loss of nigrostrial neurons and DA depletion.
Cardinal Features
• Bradykinesia
• Postural instability
• Resting tremor (may have postural and action components)
• Rigidity
Motor Symptoms
• Decreased dexterity (lack of mental skill or quickness)
• Dysarthria (speech disorder)
• Dysphagia (difficulty in swallowing)
• Festinating gait
• Flexed posture
• “Freezing” at initiation of movement
• Hypomimia- mask like face
• Hypophonia- soft speech
• Micrographia- small cramped hand writing
• Slow turning
• Autonomic Symptoms
• Bladder and anal sphincter disturbances
• Constipation
• Diaphoresis
• Orthostatic blood pressure changes
• Paroxysmal flushing
• Sexual disturbances
• Mental Status Changes
• Bradyphrenia- slowness of thought
• Confusional state
• Dementia
• Psychosis (paranoia, hallucinosis)
• Sleep disturbance
• Fatigability
• Oily skin
• Pedal edema
• Seborrhea (excessive discharge from the sebaceous glands, forming greasy scales on the body)
Treatment of Parkinsonism
• Primarily at providing maximal relief of symptoms and maintaining the independence and movement
• Successful treatment involves a total program of drug therapy, physical therapy, psychological support, and occasionally surgery
Surgical therapy- Most effective surgical technique is deep brain stimulation (DBS) of the STN, which decreases outflow from this region and reduces input to the thalamus.
Drugs are classified as follows:
ü Drugs which increase the dopamine levels
ü Anticholinergics
ü Anti histamines
ü Dopamine agonist
Non Pharmacological Therapy
• Well balanced high fiber diet
• Psychotherapy
• Physical therapy
• Speech therapy
Summary
• Many theories have been proposed & each in succession has been abandoned because of lack of supporting evidence.
Ø Neurotoxins highly selective for substantia nigra pars compacta (SNc) dopaminergic neurons –
§ 6-hydroxy dopamine
§ MPTP(N-methyl 4-phenyl tetrahydropyridine)
Ø Cellular damage from oxyradicals.
Ø Dopamine – free radicals from autooxidation and from MAO metabolism
• Cardinal Features of PD: Bradykinesia, Postural instability, Resting tremor (may have postural and action components), Rigidity

I am now 59. With the new herbal medicine for Parkinson I purchased from Multivitamincare . org was my only way to get rid of my PD,the herbal formula effectively reversed my condition and alleviated all my symptoms, people are suffering from this Parkinson disease due to lack of information.