Post Views: 128
Congestive Heart Failure

Congestive Heart Failure
Congestive heart failure (CHF), or heart failure, is a condition in which the heart is unable to pump sufficient blood to meet the metabolic demand of the body and also unable to receive it back because every time after a systole.
Classification of CHF
1. BY EJECTION FRACTION
Reduced ejection fraction(<40-50%)- systolic heart failure
Preserved ejection fraction(>40-50%)- diastolic heart failure
2. BY TIME COURSE
Chronic heart failure(CHF)
Acute heart failure (Cardiogenic Shock)
3. ANATOMICALLY
Left sided- LHF
Right sided- RHF(CHF)
4. BY OUTPUT
High output failure-Thyrotoxicosis, Paget’s disease, Anemia, Pregnancy, A-V fistula
Low output failure
Sign & Symptoms of CHF
- Shortness of breath (dyspnea)
- Fatigue and weakness
- Swelling in your legs, ankles and feet
- Rapid or irregular heartbeat
- Reduced ability to exercise
- Persistent cough or wheezing with white or pink blood-tinged phlegm
- Increased urinate at night
- Swelling of your abdomen
- Weight gain from fluid retention
- Lack of appetite and nausea
- Difficulty concentrating or decreased alertness
- Sudden, severe shortness of breath and coughing up pink, foamy mucus
- Chest pain if heart failure is caused by a heart attack
Key Indicator for Diagnosing Heart Failure
Ejection Fraction (EF)
Ejection Fraction (EF) is the percentage of blood that is pumped out of your heart during each beat.
Pathophysiology of CHF
Compensatory Mechanisms
• Sympathetic nervous system stimulation
• Renin-angiotensin system activation
• Myocardial hypertrophy
• Altered cardiac Rhythm
Classification of Drugs used in CHF
1. Inotropic drugs:
(a) Cardiac glycosides: Digoxin, Digitoxin, Ouabain
(b) Sympathomimetics: Dobutamine, Dopamine
(c) Phosphodiesterase III inhibitors: Amrinone
2. Diuretics:
(a) High ceiling diuretics: Furosemide, Bumetanide
(b)Thiazide like diuretics: Hydrochlorothiazide, Metolazone, Xipamide
3. Aldosterone antagonist:
Spironolactone, Eplerenone
4. Inhibitors of Renin-Angiotensin system-
(a) ACE-inhibitors: Enalapril, Ramipril
(b) Angiotensin (AT receptor) antagonists: Losartan
5. Vasodilators-
(a) Venodilators: Glyceryl trinitrate
(b) Arteriolar dilator: Hydralazine
(c) Arteriolar + Venodilator: Sod. Nitroprusside
6. β-Adrenergic blockers:
Metoprolol, Bisoprolol, Carvedilol
7. Others-
(a) Metabolic cardioprotectives: Trimetazidine
(b) Calcium sensitizers: Levosimendan
(c) Levocarnitine
(1) Inotropic drugs
(a)Cardiac Glycosides
If a sugar molecule is joined together with a non sugar molecule by a ether linkage it is called a glycoside.
Sugar + Nonsugar = Glycoside
Digitoxose + Steroidal Lactone = Cardiac Glycoside
Leaves of Digitalis lanata provide two – DIGOXIN and DIGITOXIN, while leaves of Digitalis Purpurea (Fox glove) are the major source of digitoxin.
Seeds of Strophanthus gratus provide two Active glycoside – STROPHANTHUS-G and OUABAIN, While seeds of strophanthus kombe yield primarily STROPHANTHIN-K.
Digoxin
A cardiac glycoside extracted from foxglove leaves (Digitalis sps.) is the most important Inotropic agent.
Increase the contractile force.
Particularly indicated in patients with atrial fibrillation.
MOA- Inhibits the Na+/K+-ATPase, which is responsible for Na+/K+ exchange across the muscle cell membrane ——> increased [Na+]in ——> increased [Ca2+]in —–> increased force of myocardial contraction.
• Positive inotropic effect (without increasing of oxygen consumption)
• Positive batmotropic effect
• Negative chronotropic effect
• Negative dromotropic effect
Extracardiac effect:
Blood Vessels- Has direct vasoconstrictor effect, there is no prominent effect on BP as it is secondary to the improvement in circulation.
Kidney- Diuresis occurs due to improvement in renal perfusion, which brings about a shift of oedematous fluid into circulation.
GIT- The effect include anorexia, diarrhea, nausea and vomiting (stimulation of CTZ)
CNS Effect- These include disorientation, hallucination (in elderly), visual disturbance and aberrations of colour perception.
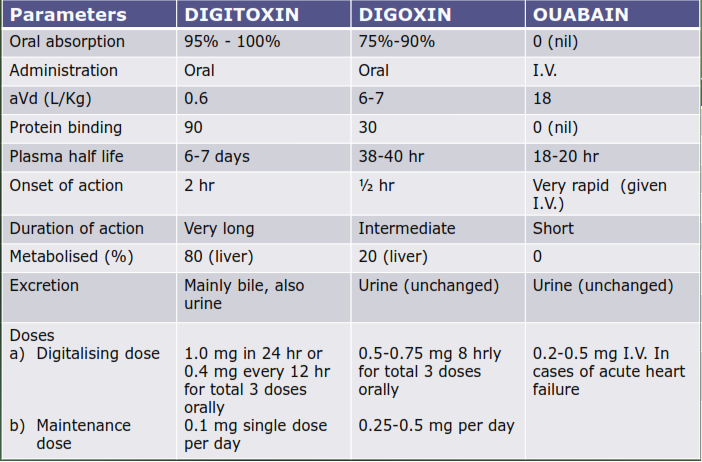
Pharmacokinetic profile of three typical cardiac glycosides
Therapeutic uses
1) Congestive heart failure- Drug of choice for “low out put HF” due to HT, IHD or arrhythmias.
2) Paroxysmal supraventricular tachycardia- it’s a arrhythmia due to reentry phenomenon taking place at SA or AV node. They frequently respond to digitalis favorably, because of reflux vagal activation which slow the conduction of impulses.
3) Atrial Flutter and Atrial Fibrillation- As it decreases conduction velocity and increases ERP of AV node.
4) Dilated Heart-As it is helpful in restoring cardiac compensation.
Side effects
Extracardiac Side effects
• GIT- Anorexia, nausea, vomiting, diarrhoea and abdominal cramps.
• CNS- Headache, fatigue, neuralgia, blurred vision, loss of colour perception.
• Endocrinal- Gyanecomastia in males (very rare)
Management of extracardiac side effects requires no more than reducing the dose of digoxin.
Cardiac side effects and Management of toxicity:
Include bradycardia, partial or complete heart block, atrial or ventricular extrasystoles, coupled beats, ventricular fibrillation and fatal cardiac arrhythmias.
If severe intoxication- administration of digitalis antibodies, e.g., Digibond Fab fragments (Digitalis immune Fab.)
These antibodies are raised against digoxin. These also recognize digitoxin and Ouabain
Contraindications:
Hypokalemia
renal impairment
MI- When HF is accompanied with atrial flutter & fibrillation
Hypothyroidism
Myocarditis or grossly damaged myocardium
Hypomagnesemia
Hypercalcemia and
Pulmonary disease
Ventricular fibrillation
Patient must be advised not to take nonprescription cough or cold medications, antacids, laxatives, or antidiarrheals without consulting the physician.
Pregnancy
(B) Sympathomimetics
They improve cardiac performance through positive inotropic effect and lead to an increase in intracellular cAMP which results in the activation of protein kinase.
Slow Ca2+ channels are then phosphorylated by protein kinase which increases Ca2+ flow into the myocardial cell causing increased force of contraction of heart muscles.
Dobutamine
The most commonly used inotropic agent other than digitalis.
On heart, dobutamine has more selective inotropic than chronotropic effect without any significant change in peripheral resistance and BP.
Its half life is about 2 min and therefore must be given by I.V. (5-10 µg/kg/min.)
It ↑ CO, therefore urinary output, and stroke volume with affecting HR, TPR or BP.
Tolerance may develop on repeated use.
As it ↑ BP it should be avoided in patients with history of HT.
Dopamine
When given by I.V. infusion in low dose (2-5 µg/kg/min.) acts on D1 receptor in kidney and causes dilatation of renal blood vessels increasing GFR, renal blood flow and urinary output.
In therapeutic doses (5-10 µg/kg/min.), also stimulate β1 receptors increasing CO but the TPR is unchanged.
In high doses (above 10 µg/kg/min.) it then activates α1 receptors also, which causes vasoconstriction with an increase in TPR and pulmonary pressure.
Adverse effects include nausea, vomiting, tachycardia, ectopic beat, HT in high dose.
(C) Phosphodiesterase III inhibitors
Amrinone and Milrinone are the two phosphodiesterase inhibitors.
They inhibiting the enzyme phosphodiesterase, increase the stay cAMP with in the myocardial cell as a result ——-> sustained rise of Ca2+ concentration in these cells occurs ——-> rise of cardiac contractility.
Both are also called “Inodilators” because they increase cardiac contractility and at the same time produce vasodilatation.
Thrombocytopenia is the most prominent and dose related side effects, but is mostly transient and asymptomatic.
Nausea, diarrhoea, abdominal pain, liver damage, fever are the other side effects.
Dose
Amrinone: 0.5 mg/kg bolus inj. Followed by 5-10 µg/kg/min. IV infusion (Max. 10 mg/kg in 24 hr.)
Milrinone: 50 µg/kg IV bolus followed by 0.4 – 1.0 µg/kg/min. infusion.
2. Diuretics
They generally cause natriuresis and water removal ——> this leads to removal of fluid from the body ——> leading to reduction of volume of blood + other ECF components (= reduction of overload) reduction of ——>
Pulmonary congestion (dyspnea) + Peripheral congestion (peripheral edema) + Preload
High ceiling diuretics – (FUROSEMIDE, BUMETANIDE)
High ceiling diuretics act principally on the ascending limb loop of Henle.
They are high potency diuretics and are effective even when there is renal insufficiency.
IV furosemide promptly increases systemic venous capacitance and produces rapid symptomatic relief in acute left ventricular failure.
Adverse effects- Acute fluid loss, hypotension, Hypokalemia, Hypomagnesimia, Hyperuricemia, Ototoxicity
Dose- Furosemide (LASIX): 20-80 mg, tab. orally
Thiazide diuretics – (Hydrochlorothiazide)
Act principally on the early distal tubule of the nephron and are of moderate potency.
Thiazide diuretics become inefficient in presence of renal insufficiency.
Thiazide however cannot be used where the GFR is < 50 ml/min.
AEs- Hypokalemia, Metabolic defects, Volume depletion, Hypersensitivity reaction.
Dose- Hydrochlorothiazide (Esidrex) 25-100 mg/day
3. Aldosterone antagonist –
(Spironolactone, Eplerenone)
These enhances Diuresis by promoting Na+ and Water excretion (While retaining K+) and prevents Myocardial as well as vascular fibrosis which is responsible for pathological remodeling of the heart.
AEs: Hyperkalemia is a major risk during the therapy and require serum K+ monitoring. Gynaecomastia may occur in male patients, after long term use.
Dose: 25-50 mg OD orally
4. Inhibitors of Renin-Angiotensin system
ACE inhibitor
These drugs not only block the conversion of Ang-I to Ang-II but also prevent the breakdown of bradykinin to vasodilatation.
They also decrease aldosterone secretion and hence reduce salt and water retention, so CO improves.
They also cause natriuresis and most imp.
They Prolong the survival by preventing pathological remodeling of the heart and blood vessels.
Most commonly used ACEIs
Enalpril (2.5 mg BD and worked up to 10 mg BD)
Lisinopril (2.5 – 5 mg OD, worked up to 20 mg OD)
Ramipril (2.5 mg OD, worked up to 10 mg OD)
AEs- Hypotension after first dose, dry cough, angioneurotic oedema, foetal hypotension with a risk of foetal malformation if administer during II or III trimester of pregnancy, hyperkalemia.
DIs- Non systemic antacid reduce the BA of ACEIs, NSAIDs may impair the hypotensive effects of ACEIs by blocking bradykinin-mediated vasodilatation etc.
Angiotensin (AT1 receptor) antagonists
Losartan
ARAs stimulate renin release and increases circulating Ang II levels, resultant increased amount of Ang II would now stimulate AT2 receptor which are lying unblocked causes vasodilatation.
Dose- 25-50 mg OD
AEs-
Cause foetal toxicity
Precipitate renal failure in patients with bilateral renal artery stenosis.
Hyperkalemia in patients with renal failure First dose hypotension in rare cases may occur
5. Vasodilators
These agents reduce pulmonary congestion and increase cardiac out put by reducing preload and/or after load.
They also prevent remodeling of the heart.
The nitrate receptors presents on smooth muscle.
The nitrate receptors possess –SH groups which reduce nitrates to nitrite and nitric oxide (NO).
The NO itself gets converted to an intermidiate- reactive nitorsothiol which activates intracellular guanylate cyclase (GC) to convert GTP to cGMP results in vascular smooth muscle relaxation.
Nitorglycerine
In patients of HF with dyspnoea, venodilators like or long-acting nitrates are preferred because these may reduce the filling pressure and ultimately the pulmonary congestion.
Dose-
Route Dose (mg) Onset (min) Duration (hrs)
Sublingual 0.5 2-5 0.25-0.5
Oral 5-15 20-30 4-8
Ointment (2%) – 15-30 3-8
Transdermal 5-10 mg/24hr 30-40 Max. 24 hr
AEs- Throbbing headache, flushing of face, palpitations, dizziness, Tolerance develop rapidly if used orally in sustained release form, or transdermally or by I.V. infusion without drug free interval.
DIs- Sildenafil and other vasodilator potentiate the hypotensive action of nitrates (Inhibit the metabolizing enzymes PDE-IV and potentiate further release of cGMP), sudden death occures.
Arteriolar dilator
Hydralazine
Vasodilatation due to hydralazine is partly endothelium dependent and may involve generation of nitric oxide and stimulation of cGMP, increase in intracellular levels of cGMP are associated with vascular smooth muscle relaxation.Hydralazine (25-50 mg BD orally) and is generally not employed BY I.V. route because the onset of action is hardly different than that of oral
AEs- Headache, tachycardia, nausea, nasal congestion, and anginal attack (due to tachycardia), prolong use in High doses it causes reversible disseminated lupus erythematosus like syndrome
Arteriolar + Venodilator
(Sod. Nitroprusside)
Sod. Nitroprusside activates guanylyl cyclase either directly or through release of nitric oxide.
This results in an increase in the intracellular levels of cGMP which provides vascular smooth muscle relaxation.
Patients having severe chronic failure benefitted by combination of arteriolar + venodilator, And useful in patients in whom ACEIs are contraindicated or are not tolerated.
Dose- It is powerful parenterally administered vasodilator, the onset effect is rapid (30 sec.) after I.V. infusion (0.3 µg/kg/min, slowly raised to 0.5 µg/kg/min) and disappear within 10 min after discontinuation.
AEs- Other than headache, nausea and vomiting Which quickly dissipate after the infusion is stopped.
6. β-Adrenergic blockers:
Metoprolol, Bisoprolol, Carvedilol
As a general rule β- blockers are contraindicated in CHF.
Because HF patients have a decreased CO since CO is equal to stroke volume (SV) multiplied by heart rate (HR), an increase HR would be necessary to maintain an adequate CO in the presence of decreased SV as observed in HF.
As a result, a decrease in HR and cardiac contractility produced by β- blockers would be expected to produce acute cardiac decompensation, in patients with HF.
β- blockers like Metoprolol, Bisoprolol, carvedilol, improve ventricular function and prolong the survival in HF patients.
Doses-
Metoprolol- 50-100 mg OD orally
Bisoprolol- 2.5-10 mg OD orally
Carvedilol- 6.25 mg BD orally, increased to 12.5 mg BD
AEs-
Bronchoconstriction
Sudden withdrawal of β- blockers is very dangerous most imp. Cause seems to be up regulation of β- adrenoceptors due to use of β- blockers.
Person who use insulin or oral antidiabetic tab. Are susceptible to develop hypoglyemia.
Occasionally can produce some CNS symptoms like depression and sleep disturbance.
Rash, urticaria rarely.
Can mask some symptoms of hyperthyroidism.
Absolute CIs- Severe bradycradia, pre existance gross block in the conducting system and overt left ventricular failure, Asthma, COPD, Depression, Active peripheral vascular disease.
7. Other drugs
Metabolic cardioprotectives: Trimetazidine
It prevents the degradation of membrane unsaturated fatty acids by lipid peroxidation and
thus reduce myocardial O2 demand.
It also inhibit the superoxide cytotoxicity to protect the myocardium from the harm full effect. but can cause parkinsonism.
Dose- 20-60 mg OD tab. and cap.
Calcium sensitizers
Levosimendan
It increases sensitivity of troponin in the Heart to calcium.
This results in increased myocardial contractility.
It is infused i.v. for short treatment of severe heart failure.
Levocarnitine
It is a N-containing amino acid in muscle, which has antioxidant activity. It is indicated in cardiomyopathy and muscle dystrophy caused by carnitine deficiency.
Preparations containing Coenzyme Q10 (a part of the mitochondrial redox system), stimulate ATP synthesis and improve myocardial contractility in CHF.
Non Pharmacological
Activity
Routine modest exercise for class I-III– For euvolemic patients
Regular isotonic exercise such as walking or riding a stationary-bicycle ergometer
Diet
Restriction of sodium (2-3 g daily) is recommended in all patients, Extra < 2g reduction in moderate to severe cases.
Fluid restriction (<2 L/day) if hyponatremia (<130 meq/L)
Caloric supplementation- with advanced HF and unintentional weight loss or muscle wasting (cardiac cachexia)
Reduce or eliminate alcohol and caffeine
Quit Smoking
Surgical measures
Cardiac Resynchronization
Implantable Cardiac Defibrillators
Intraaortic balloon counter pulsation
Percutaneous and surgically implanted LV assist devices
Biventricular Pacing
Cardiac transplantation
Novel agents in HF
Newer InotropeS
– Cardiac myosin activators- Omecamtive mecarbil
– Na/K-ATPase inhibitors- Istaroxime
– Ryanodine receptor stabilizers- JTV-519(K 201),S107,S44121
– SERCA2a activators- MYDICAR
Vasodilators- Relaxin
Neuregulins- recombinant human NRG-1β2
Novel RAAS blockers-
– Direct renin inhibitors- Oral Aliskiren,IV Remikiren, IV Enalkiren
– Angiotensin receptor & neprilysin inhibitors- LCZ696, AHU377 ,Candoxatril, Ecadotril
– Aldosterone blockers –
Dual ACE/NEP Inhibition – Vasopeptidase Inhibitors
Dual NEP & ECE(endothelin converting enz.) inhibitors – GGS34043, GGS34226, GGS26303, SLV306
Triple enzyme inhibitors of ECE/NEP/ACE – GGS26670
Dual dopamine D2-α2 agonist – Nolomirol
Dopamine β-Hydroxylase inhibitor – Nepicastat
Adenosine A1 receptor antagonists – BG9719,BG9928
Carnitine palmitoyl transferase-1(CPT-1) inhibitors – Etoxomir, Oxenicine
Matrix Metalloproteinase (MMP) Inhibitors– Batimastat, ilomastat, marimastat and prinomastat
Immune modulator – CelacadeTM
Cardiac Myosin Activators
(Omecamtive Mecarbil)
They accelerate transition of actin-myosin complex from a weakly bound to strongly bound configuration
↓
↑ myosin head interaction with actin ↓ nonproductive ATP hydrolysis
↓
↑duration of systole —-> ↑stroke vol – —->improvement
in myocardial systolic function in absence of arrythmogenesis & ↑ O2 consumption.
Currently under phase 2 trial.
Istaroxime
MOA-
Inhibition of sodium/potassium adenosine triphosphatase (Na+/K+ ATPase).
Drug is under phase 2 trial.
Vasodilators – Serelaxin
Recombinant human relaxin- 2
Relaxin- circulating peptide found in pregnant women
Regulates systemic vasodilation
Improves dyspnea significantly
Dose 30 μg/kg/day infusion
Currently under phase 3 trial.
SERCA 2a activators
Improved systolic and diastolic functions, improved ventricular metabolic reserve, and reducing the likelihood of ventricular arrhythmias during ischemia-induced Ca2+ overload
Currently under phase 3 trial.
Ryanodine receptor stabilizers (JTV519 )
preserve left ventricular systolic and diastolic function
prevents left ventricular remodeling
Neuregulins
Recombinant human NRG-1β2 infusion improve cardiac structure and function by 90 days
Increase in cardiac output as well as vasodilator effect
Currently under phase 3 trial.
Novel blockers of the renin–angiotensin aldosterone system
Direct renin inhibitors
Oral Aliskiren,IV Remikiren, IV Enalkiren
Reduce increased plasma renin activity directly independent of plasma levels of BNP, background effect of beta blockers & ACEI.
MOA- inhibit conversion of Angiotensinogen to angiotensin-I
Drawback- hyperkalemia, hypotension
Angiotensin receptor and neprilysin inhibitors
(Candoxatril, Ecadotril)
Atrial natriuretic peptide, B, C and exogenous D- type, possess differing degrees of hemodynamic, neurohormonal, renal and cardiac effects
Novel approaches to aldosterone blockade Non-steroidal mineralocorticoid receptor antagonists
PF3882845 -greater blood pressure reduction and renal protection
BR-4628 -dihydropyridine (DHP) structure
Aldosterone synthase inhibitors
There is induction of aldosterone synthase (CYP11β2) or angiotensin II in the failing ventricle
FAD286 – improved cardiac hemodynamic parameters, preventing progressive LV remodeling
LCI699 – reduction in blood pressure
Triple Enzyme Inhibitors of ECE/NEP/ACE
GGS 26670
Improved LV function and reduced LV collagen accumulation better than either ACE alone or ECE-NEP inhibition
Dual Dopamine D2- Adrenoceptor agonist
Nolomirole
Inhibits catecholamine release from sympathetic nerve endings and also inhibits the release of TNF from cardiac tissue
Significantly reduces hypertrophy and attenuates signs and symptoms
Dopamine-Hydroxylase Inhibitor
DBH catalyses the conversion of dopamine (DA) to norepinephrine (NE) in sympathetic nerves
Nepicastat- reduce norepinephrine synthesis.
Phase 2
Adenosine A1 receptor antagonists
BG 9928, BG 9719
Protects renal function and exerts additive natriuretic effects without excessive potassium loss
Carnitine Palmitoyl Transferase-1 (CPT-1) Inhibitors
CPT-1 helps in metabolism of fatty acid which is a source of energy production in heart
Etoxomir, Oxfenicine
dilation, prevents ventricular remodeling.
Matrix Metalloproteinase (MMP) Inhibitors
Enhanced expression of MMP triggers signaling cascade of cardiac remodeling
Batimastat, ilomastat, marimastat and prinomastat, PG-53072
Prevent ventricular dysfunction and delay heart failure progression
Immune modulator
CelacadeTM
Prevents chronic inflammation and apoptotic cell death by activating physiological immune system’s IL -10 mediated anti-inflammatory process.
Improve quality of life in patients of NYHA class III or IV heart failure.
Reduce the risk of death and hospitalization due to chronic heart failure
Can CHF prevented
CHF can’t always be prevented, but there are many things can do to help.
Try preventing CHF by practising good heart health.
This will also guard against heart attack, stroke, and coronary artery disease.
Tips to follow include:
Control high blood pressure
Eat a healthy diet• Exercise
Control blood sugar levels (especially if you have diabetes)
Maintain good blood cholesterol levels
Quit smoking
Drugs Used in Congestive Heart Failure Notes PDF